vHIT: A Comprehensive Overview
What is the Video Head Impulse Test (vHIT)?
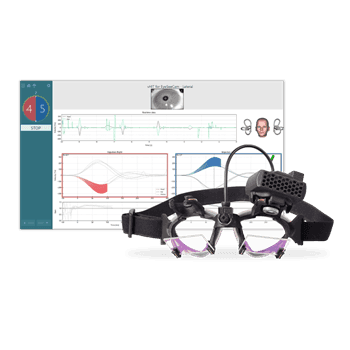
The vHIT is an advanced assessment to diagnose asymmetries in vestibular function between the ears. By using lightweight video goggles, vHIT measures eye velocity and detects any abnormalities. This allows hearing health professionals to quickly and objectively assess the Vestibulo-Ocular Reflex (VOR) in response to natural head movements.
Through precise measurement of left or right eye velocity during head impulses, vHIT provides data on the VOR’s performance, enabling accurate diagnosis of vestibular deficits. This instrumented technique is essential for understanding a patient’s vestibular health and guiding effective treatment strategies.
What Does the vHIT Diagnose?
vHIT records eye movements in response to rapid head rotations across different planes. This enables a comprehensive evaluation of all six semicircular canals in the inner ear, providing an objective measure of VOR function and helping to pinpoint potential inner ear issues that might cause dizziness.
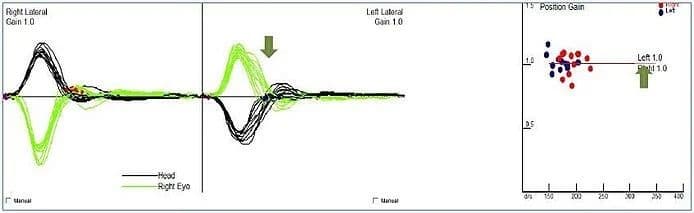
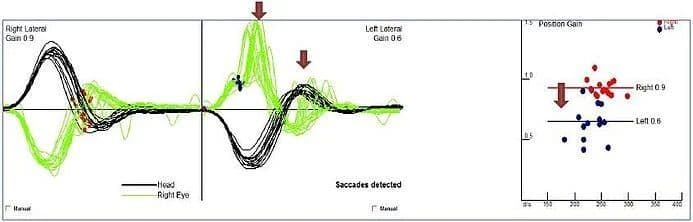
By assessing the VOR and its ability to maintain gaze during head movements, vHIT can identify weaknesses in one or both vestibular systems.
This information proves crucial for diagnosing various conditions that can disrupt balance, including vestibular neuritis, benign paroxysmal positional vertigo (BPPV), Meniere’s disease, and even central nervous system disorders that impact the vestibular pathways.
vHIT vs. Traditional Bedside Head Impulse Testing
While traditional bedside head impulse testing (HIT) has served as a valuable tool, it presents limitations. HIT relies on visual observation of corrective saccades, involuntary eye movements that maintain fixation on a target despite head motion. HIT struggles to detect covert saccades - corrective movements that occur during the head impulse itself, leading to missed diagnoses.
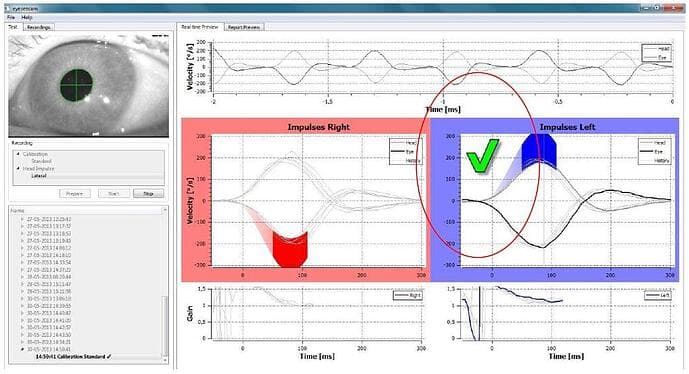
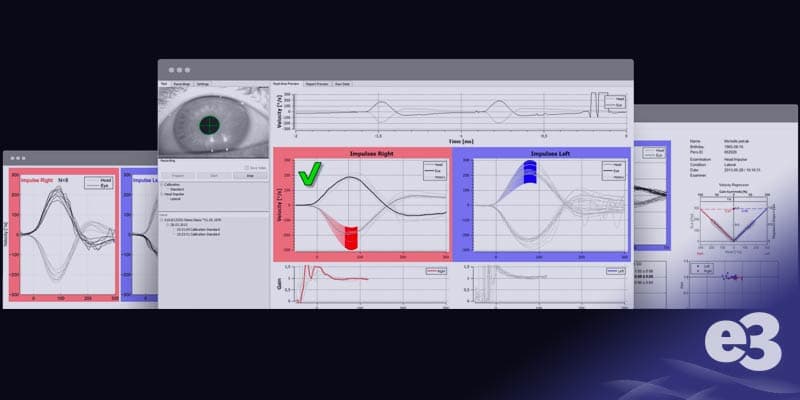
vHIT addresses these limitations by incorporating sophisticated technology. During vHIT testing patients wear specialized goggles equipped with infrared cameras that precisely track eye movements during rapid, controlled head rotations in various planes.
By capturing and analyzing both overt and covert saccades, vHIT provides quantitative data on corrective saccades, enhancing diagnostic accuracy for inner ear dysfunction potentially contributing to dizziness.
This objective data empowers healthcare professionals. vHIT results can inform referrals, supplement information from other tests, and ultimately contribute to more precise treatment plans for patients experiencing balance issues.
The Vestibulo-Ocular Reflex Explained
The Vestibulo-ocular reflex is the connection between the vestibular system and the oculomotor muscles. A normal functioning VOR allows for visual fixation in the presence of head movement. Visual fixation or gaze stabilization is necessary because images must stay long enough on the retina to be encoded into neural signals. Otherwise, everything will appear blurry during head movement, and we would be unable to have clear vision.
To achieve a steady retinal image during head motion, the information from the peripheral vestibular system is passed to the ocular pathways, where compensatory eye movements are generated by moving the eyes with the same velocity in the opposite direction of the head movement.
The VOR comprises of three components; the vestibular organs in the cochlea, the central processing mechanism, and the motor output to the eye muscles. (Fetter, 2007)
The semicircular canals (SCCs) and the otolith organs sense angular and linear movement, respectively. The SCCs are arranged in pairs based on the plane of activation and have a push-pull relationship. The two lateral canals are in the same plane and respond together to angular head movement.
A head turn to the right, for example, results in ampullopetal endolymph flow (towards the ampulla) in the right ear, which results in an excitatory neural response, and ampullofugal endolymph flow (away from the ampulla) in the left ear, which is inhibitory.
Similarly, the anterior canals and the contralateral posterior canals function in pairs. When head movements elicit an excitatory response on one side, the paired canal on the contralateral side produces an inhibitory response.
As the cochlea responds to head movement, information is sent to the central processing mechanism via the superior and inferior branches of the vestibular nerve. From the central processing mechanism, information is sent to the ocular muscles to produce reflexive eye movement in the opposite direction of the head movement but at the same velocity.
Evaluating the Vestibulo-Ocular Reflex
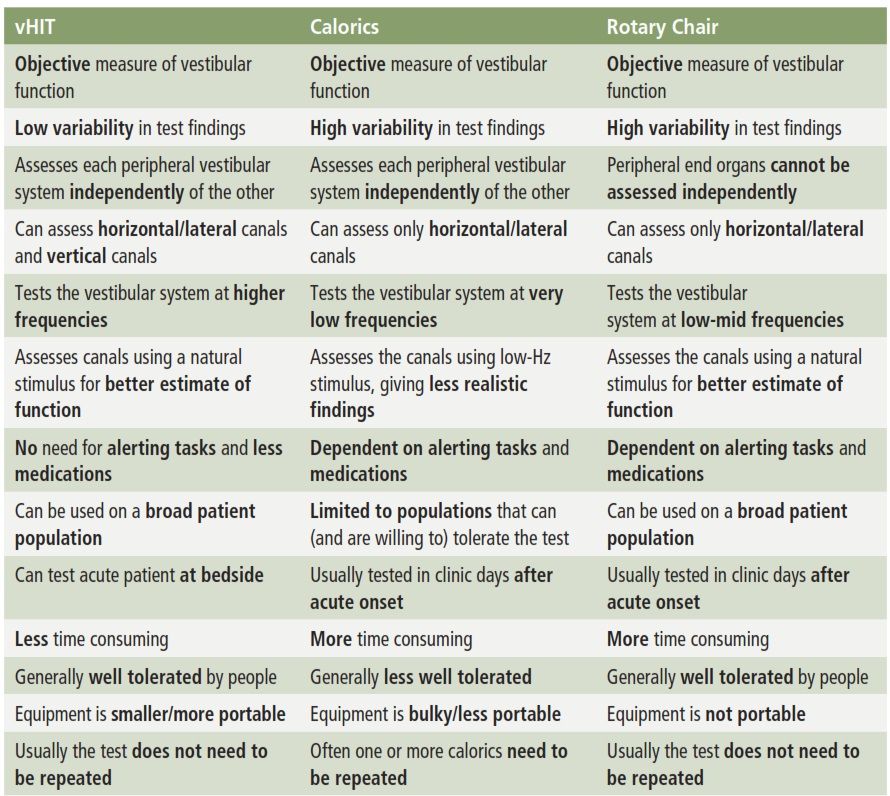
Traditionally, audiologists have evaluated the VOR with caloric stimulation during the VNG and with rotary chair testing. During the caloric test, warm stimulation results in ampullopetal flow of the endolymph which yields an excitatory response and nystagmus that beats toward the stimulated ear.
Cool caloric stimulation results in ampullofugal endolymph flow and nystagmus that beats away from the stimulated ear. During rotary chair testing, rotating the patient to the right or left yields the same response as the head turns described earlier. There are limitations to these procedures, however.
Natural head movements in humans range from 0.1 to 10 Hz. Caloric stimulation, while it provides objective and measurable responses, evaluates the VOR at 0.003 Hz, which is much slower than natural movements. (Turning at 0.003 Hz is analogous to taking roughly four minutes to rotate 360 degrees.) Rotary chair evaluates the VOR at higher frequencies, but still only up to 0.64 Hz. This leaves much of the range of natural head movement unevaluated.
Additionally, the superior branch of the vestibular nerve innervates the lateral and anterior SCCs and the inferior branch innervates the posterior SCC. If we are only looking at the function of the lateral canal with VNG and rotary chair, we lack information on the function of the inferior branch of the vestibular nerve.
Contribution of vHIT to the VOR evaluation
Video head impulse testing fills in the gaps left by the traditional test protocols. Like VNG and rotary chair testing, vHIT provides information on the lateral SCCs, but it does so by assessing the system at frequencies between 3 and 6 Hz which are much more representative of natural head movements. It is also possible to perform head thrusts in each plane of the three pairs of SCCs to obtain information on all six canals and both branches of the vestibular nerve.